Urinary incontinence is an uncontrolled leak of urine which can be very distressing and embarrassing for an adult. It is more common in women but elderly men may suffer too. There are several causes for incontinence including overactive bladder, stress incontinence and overflow incontinence. Diagnosis requires a careful discussion and examination of the patient followed by diary records, ultrasonography and, in select patients, urodynamics evaluation. It is almost always possible to make a patient dry by a combination of lifestyle changes, medication and occasionally surgery. Some individuals with urinary incontinence may be suffering from a different medical condition called neurogenic bladder. It is crucial to identify individuals with neurogenic bladder since their management is entirely different.
Overactive bladder & Urge Incontinence
Overactive bladder is a distressing lifestyle problem that can afflict both men and women. Women with overactive bladder are more likely to have difficulty controlling the leak (the so-called OAB-wet). Overactive bladder is presumably due to an ‘irritability’ of the bladder (detrusor overactivity) but there are many individuals in whom such irritability cannot be demonstrated. Excessive fluid intake can aggravate the symptoms. Diagnosis rests on a careful clinical assessment to rule out other causes of the symptoms, preparation of 24hr diary records, ultrasonography and rarely urodynamics. Treatment consists of lifestyle changes, fluid restriction, use of anticholinergic medication and pelvic floor training. In some patients one may have to resort to more aggressive treatments such as botulinum toxin injections into the bladder wall or rarely even surgery.
Dr KVR Prasad was invited by the South African Urogynecological Association in 2008 to conduct an International workshop on overactive bladder. He has demonstrated botulinum toxin injection in a live operative workshop at Post Graduate Institute Chandigarh PGIMER in 2009.
Post-prostatectomy Incontinence
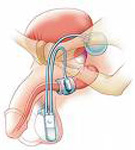
Urinary incontinence following prostatectomy surgery can be devastating for the patient. This usually follows operation for cancer (radical prostatectomy) but can rarely occur after endoscopic surgery for benign disease (TURP). Pelvic exercises, fluid management, medication and a allowing a few months to pass by may help. However for severe incontinence the only really effective solution is an artificial sphincter.
Stress Urinary Incontinence
Stress urinary incontinence is a distressing condition in which women leak urine on coughing, straining or even on minimal activity such as getting up from bed. The condition is common and can be diagnosed by a clinical evaluation combined with ultrasonography. In most patients, a urodynamics test (test for bladder function) is recommended prior to any surgical intervention. In women who opt for surgical correction, placement of a synthetic tape is the procedure of choice. Such tapes can be placed by a minimally invasive approach either through the lower part of the abdomen (retropubic tapes such as TVT or Sparc) or from below (by a transobturator approach). In some women, one may opt for an autologous rectus fascia sling fashioned out of the woman’s own tissues. This may be preferable in women with very poor urethral function or those with prior failed procedures with an unhealthy vagina.